Awake craniotomy for tumour
Awake craniotomy is an operation designed to facilitate surgical access and resection of tumours located in parts of the brain that control important functions, like movement, speech (understanding, repetition, expression of speech, precise formation of sentences, naming), reading, visual fields. Awake craniotomy is carried out by oncological neurosurgeons who had training and have acquired experience in this type of surgery. Neurosurgeons work closely with neuro-anaesthetists who have an interest and have acquired experience in awake surgery. The role of the anaesthetist during an awake operation is of immense importance. The anaesthetist is able to modify the level of sedation of the patient (from fully alert to almost anaesthetised), so the surgical plan is facilitated. In the event of a prolonged intraoperative seizure, that cannot be controlled with conventional measures the anaesthetist secures the patient's airway and might need to anaesthetise the patient so the seizures are controlled.
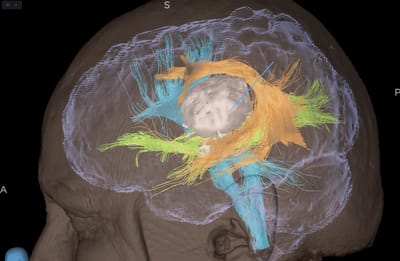
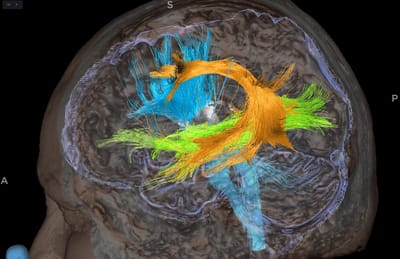
The intraoperative assessment of the patient during an awake craniotomy is carried out by a neuroscientist or the anaesthetist (depending on the case). The intraoperative assessment in an awake craniotomy is based on continuous assessments to establish whether the patient is able to perform certain tasks depending on the location of the tumour and the stage of the operation. All this is planned virtually on workstations before the operation. Using data from the patient's preoperative imaging we are able to create 3d models of the tumour and its relationship with important intrinsic pathways inside the brain that control certain functions that have to be preserved during surgery. This technology allows us to establish whether resection of the tumour is possible and quantify the risk of the operation as best as possible. The example images attached in this section are an example where complete resection could not be possible due to the close relationships of the tumour with pathways controlling speech and movement. However, a subtotal but significant resection was considered possible and achieved on the day of the operation.
Patient usually tolerate awake craniotomies very well. The technique is based on the principle that the brain does not have any pain sensors. After local anaesthesia is administered to anaesthetise the scalp, an operation can take place in the brain with minimal or no pain. However certain structures/locations in the brain can cause if touched during the procedure, Neurosurgeons and and neuro-anaesthetists are aware of this and avoid these structures when the patients are fully alert.
Awake craniotomies, carried by the correct team, have revolutionised the management of brain tumours which in the past were labelled as inoperable or were associated with high postoperative morbidity and mortality.
The intraoperative assessment of the patient during an awake craniotomy is carried out by a neuroscientist or the anaesthetist (depending on the case). The intraoperative assessment in an awake craniotomy is based on continuous assessments to establish whether the patient is able to perform certain tasks depending on the location of the tumour and the stage of the operation. All this is planned virtually on workstations before the operation. Using data from the patient's preoperative imaging we are able to create 3d models of the tumour and its relationship with important intrinsic pathways inside the brain that control certain functions that have to be preserved during surgery. This technology allows us to establish whether resection of the tumour is possible and quantify the risk of the operation as best as possible. The example images attached in this section are an example where complete resection could not be possible due to the close relationships of the tumour with pathways controlling speech and movement. However, a subtotal but significant resection was considered possible and achieved on the day of the operation.
Patient usually tolerate awake craniotomies very well. The technique is based on the principle that the brain does not have any pain sensors. After local anaesthesia is administered to anaesthetise the scalp, an operation can take place in the brain with minimal or no pain. However certain structures/locations in the brain can cause if touched during the procedure, Neurosurgeons and and neuro-anaesthetists are aware of this and avoid these structures when the patients are fully alert.
Awake craniotomies, carried by the correct team, have revolutionised the management of brain tumours which in the past were labelled as inoperable or were associated with high postoperative morbidity and mortality.